All people have unique anatomy (the way your bones, joints, muscle and soft tissues are made). Mako Robotic arm assisted surgery references your unique anatomy in order to plan and implement a patient specific knee replacement.
Enhanced Patient Specific Planning:
Before surgery a CT scan is performed on your knee joint. To help understand your unique alignment, your hip and ankle are also scanned. The information obtained from this CT scan allows for a 3-Dimensional model of your knee joint to be created. This allows the surgeon to pre-operatively plan the size and orientation of your knee replacement.
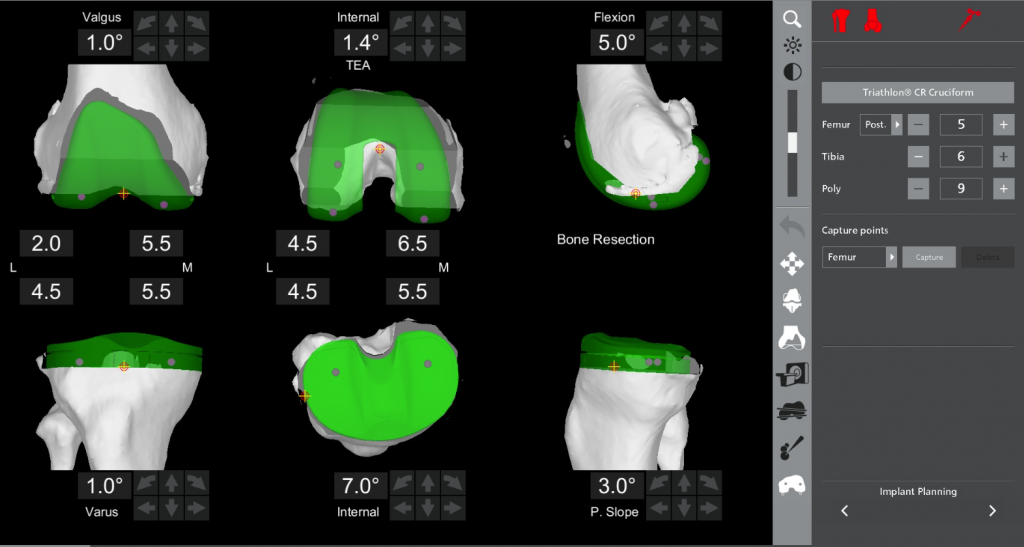
Functional Implant Positioning
During surgery your knee joint is placed through a range of movement and the overall alignment, ligament tension and the way the knee moves is assessed. Precise movements of the knee replacement components can then be made to best match your anatomy. The robotic software provides real time information to allow accurate implant positioning. This occurs before bone preparation occurs.
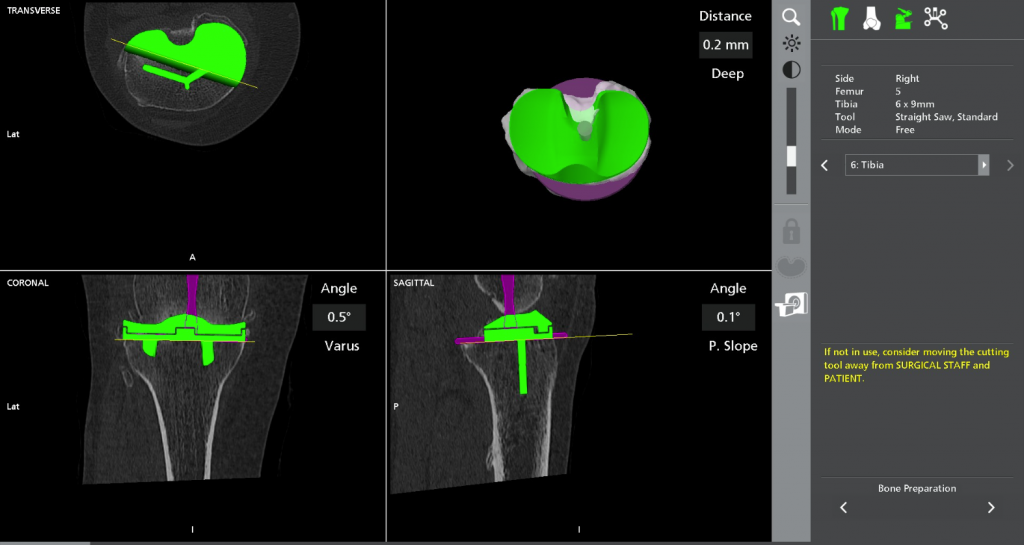
Robotic Arm Assisted Bone Preparation
The Mako Total knee application does not require cutting blocks, sizing guides or intramedullary rods for bone preparation. The surgeon controlled robotic arm creates a virtual boundary to assist with the removal of only the damaged bone and cartilage while protecting to soft tissues such as the PCL and the blood vessels and nerves at the back of the knee. It provides the surgeon with tactile feedback, 3-D visualisation and auditory guidance to facilitate precise bone removal.
Finally once all components have been implanted, a summary screen allows your surgeon to confirm that your results are accurate and according to the pre-operative plan.
Adequate soft tissue protection is achieved using Mako robotic-arm assisted surgery for Total Knee Arthroplasty. It offers protection of the medial collateral ligament (MCL), lateral collateral ligament (LCL), posterior cruciate ligament (PCL), and patellar ligament with no visible evidence of disruption of any of the ligaments. Tibial subluxation was not required for tibial cutting, which may reduce ligament stretching. All cases were left with a bone island on the tibial plateau, which protected the PCL. In addition, patella eversion was not required for visualization.(5).